
The dimly lit auditorium is crowded, boisterously loud, and smoke-filled. The raucous crowd focuses on the boxing ring brightly lit in the center of the room. An official stands in the spotlight and grabs the overhead microphone.
"Ladies and Gentlemen! In this corner, the heavyweight champion - Rock 'em Sock 'em Sjogren's Syndrome!"
The crowd cheers wildly.
"In this corner, the lightweight contender - Spittin' Sammy salivary gland!"
The platinum blonde next to you adjusts her mink wrap as the crowd jeers. She stops chewing her wad of gum long enough to lean over and comment, "Awww. Poor little guy don't have a chance.."
Unfortunately, Blondie is right. Anyone who deals with the heavyweight champ Sjogren's Syndrome knows that our saliva glands don't last long in the ring before a KO punch puts them down for the count.
Why is that? And what's so important about a salivary gland, anyway?
(Julia rolls out an overhead projector and dims the lights.)
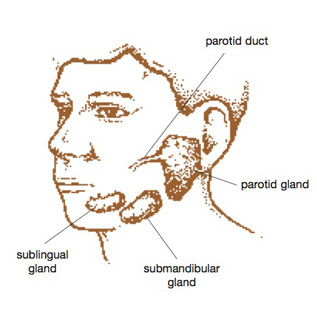
Everyone has three sets of salivary glands - the parotid in front of your ear, the submandibular under your jaw, and the sublingual under your tongue. These glands are responsible for secreting saliva, a very complex liquid that has several properties:

Gosh, and I used to think that saliva was mostly good for making spit balls. To smack Scott Hendrickson with. Because he tied my hair to my chair in fourth period homeroom once. Ah, the good old days.... but Sjogren's Syndrome has made my spit ball expertise a thing of the past.
In Sjogren's Syndrome, autoimmunity triggers destruction of cells which secrete fluids. This cell destruction, which also occurs elsewhere in the body, can create a multitude of problems, one of which is the significant decrease of saliva produced.
If you have Sjogren's, and don't have a copy of The New Sjogren's Syndrome Handbook edited by Steven Carsons, MD, and Elaine K. Harris, consider picking up a copy. It contains detailed information about decreased saliva production and all the other effects that SjS may have on your body. This post will focus on the dry mouth issues from Sjogren's.
The following information has been paraphrased from the Handbook:
Normal saliva has five major functions:
- Coating and lubricating the mucous membranes inside the mouth.
- Act as a cleansing mechanism to remove food remnants and potentially harmful bacteria from the teeth and soft tissues.
- Maintaining a chemically neutral pH balance in the oral cavity.
- Balance the calcium and phosphate in the teeth and decrease susceptibility of tooth decay and erosion.
- Protect oral cavity from bacterial infections and yeast (Candida) infections by utilizing salivary proteins which inhibit bacterial, yeast, and viral growth.
What seems to be the quickest and easiest solution when faced with decreased saliva production - to guzzle large amounts of water - isn't the best choice.
Plain water lacks components such as mucins (lubricating agents), buffering substances, calcium and phosphate salts, antibodies (secretory IgA), and salivary proteins.
Besides lacking important components, water, when drunk in large amounts, will not overcome mouth dryness, and may remove any remaining mucous on the lining of the mouth and further increase the symptoms of dryness. Frequent small sips of water during the day is more beneficial, and reduces the need to make trips to the bathroom during the night.
There are other treatment options for Sjogren's dry mouth.
Medications are available which stimulate salivary flow, but only in those patients who have some function remaining in their salivary glands. These drugs must be prescribed by your doctor, and may have side effects. Pilocarpine and cevimeline HCL are examples of these types of medications.
Saliva substitutes are also available, and are especially useful for those who wear dentures. These work best when used at bedtime, while talking, or traveling. They work for a limited amount of time because eventually they are swallowed, and take their beneficial properties with them.
Some patients benefit from chewing sugarless gums or letting sugarless hard candies dissolve in their mouth. Care should be taken to avoid candy and gum containing sugar, however, since sugar will promote tooth decay, a significant problem when facing a decrease in saliva.
Which brings up an important issue - prevention of caries, or cavities. For all the reasons described above, meticulous care of your teeth is vital. Good oral hygiene (there's that word again - see a previous post) such as twice daily tooth brushing with a flouride-containing toothpaste, daily use of dental floss, and avoiding sugar in the diet is a good place to start.
Unfortunately, once Spittin' Sammy the saliva gland loses his fight to Sjogren's, the cells destroyed can't be replaced. Research someday - and I hope soon - will provide a something to deliver a knock out punch to Sjogren's.




{kind=link}
4 comments:
Could you tell me what the "sialic glands" are in the body and what their function is? I googled it and was only able to find sialic acid.
Thanks!
Hi Deb - My understanding of sialic acids are that they are actually created by an enzyme, aldolase, which is found all through the body but especially in muscle tissue.
Thanks so much Julia. I am taking a Med Transcptn course into the dictation part and the mentioned "sialic glands" as part of an ENT report. G-d bless!
Not sure if this is the right place to ask.... I have been recently labeled but lip biopsy was negative. Now, wicked swelling in the parotid gland, swollen lymph nodes, drainage and icky taste. Primary care said to take a wait and see attitude. Now 8 weeks later it's hard to chew and ear has fluid behind it. Primary care prescribe clynamycn and but in referral for ENT. No fever but my face looks like a chipmunk and antibiotics haven't made any difference. Thoughts? Could this just be sjogrens swelling and it will eventually calm down?
Post a Comment